Atherosclerosis is a disease of arterial blood
vessels. Venous vessels are not involved unless surgically moved
to function as an artery. Atherosclerosis is commonly referred to
as a "hardening of blood vessels", but this is an
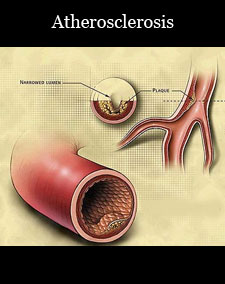
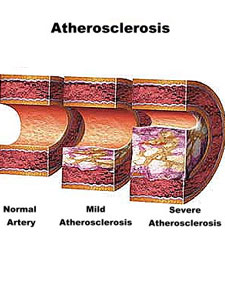
over-simplification. Vascular lesions known as atheromatous
plaques or atheromata (singular: atheroma) are formed in the
vessel wall, and in late stages may reduce or restrict blood flow
in the lumen. When the inner covering of an unstable atheroma
breaks, compromising the structural integrity of the internal
artery wall, the break may allow hemorrhage into the plaque,
generate stenosis, embolism, (very rarely even hemorrhage beyond
the artery wall), sometimes leading to severe morbidity and even
death.
The resident cells within the artery wall seem to signal an
intrusion, "call for help", an inflammation response. Monocytes,
one of the 5 main types of white blood cells circulating in the
blood, enter the artery wall. Within tissues, monocytes change
characteristics and are called macrophages. The macrophages ingest
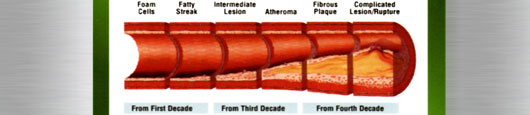
oxidized cholesterol, slowly turning into large "foam cells" – so
described because of the appearance numerous vesicles take on to
accommodate their high lipid content. The early stages are called
fatty streaks. Foam cells eventually die, and further propagate
the inflammatory process.
Intracellular micro calcification deposits form within vascular
smooth muscle cells of the surrounding muscular layer,
specifically in the muscle cells adjacent to the atheromas. In
time, as cells die, this leads to extracellular calcium deposits
between the muscular wall and outer portion of the atheromatous
plaques.
Cholesterol is delivered into the wall by LDL particles ( low
density lipoprotein), especially by the smaller LDL particles, if
they are plentiful, because they can pass through the
intracellular gaps between the intima lining cells more easily. To
attract and stimulate macrophages, the cholesterol must be
released from the LDL particles and oxidized, a key step in the
ongoing inflammatory process. Additionally, the macrophages must
be unable to remove excess cholesterol fast enough, into
functioning HDL particles ( high density lipoprotein) to avoid
becoming foam cells and dying. To date, the only known mechanism
by which macrophages can export excess lipid is into HDL
particles.
A protective fibrous cap normally forms between the fatty deposits
and the artery lining (the intima). These capped fatty deposits
(called atheromas) produce enzymes which cause the artery to
enlarge over time. As long as the artery enlarges sufficiently to
compensate for the extra thickness of the atheroma, then no
narrowing, stenosis, of the opening, lumen, occurs. The artery
becomes expanded and egg shaped, still with a circular opening. If
the enlargement is beyond proportion to the atheroma thickness,
then an aneurysm is created.
This process of atheroma formation and progressive artery
enlargement, or remodeling, usually starts in childhood and
continues for many decades, thereby masking either symptoms or any
evidence of the disease by any detection methods, such as
angiography, which only evaluate the artery lumen.
In effect, small aneurysms of the muscular portion of the artery
wall form aneurysms just large enough to hold the atheroma which
are present. The muscular portion of artery walls usually remain
strong, even after they have remodeled to compensate for the
atheromatous plaques.
However, atheromas within the vessel wall are soft and fragile
with little elasticity. Arteries constantly expand and contract
with each heartbeat, i.e. the pulse. In addition, the
calcification deposits between the outer portion of the atheroma
and the muscular wall, as they progress, lead to a loss of
elasticity, stiffening, of the artery as a whole.
The calcification deposits, after they have become sufficiently
advanced, are partially visible by some high resolution X-Ray
imaging systems as rings of increased radiographic density forming
halos around the outer edges of the atheromatous plaques, within
the artery wall. On CT, >130 units on the Hounsfield scale {some
argue for 90 units) has been the radiographic density usually
accepted as clearly representing tissue calcification within
arteries. These deposits demonstrate unequivocal evidence of the
disease, relatively advanced, even though the lumen of the artery
is often still normal by angiographic or IVUS imaging.
Although the disease process tends to be slowly progressive over
decades, in later stages, it also becomes unstable with repetitive
sudden problems, most without obvious symptoms at the time of
occurrence but some producing sudden major debility or death.
These problems result from instability of the newer, soft
atheromas.
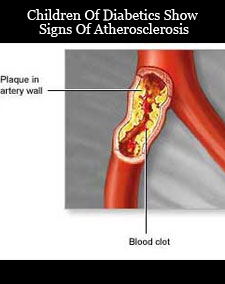
If the fibrous cap separating a soft atheroma from the bloodstream
within the artery ruptures, atheroma tissue fragments are exposed
and released. Atheroma tissue fragments are very clot promoting;
they attract blood platelet accumulation and activate the blood
clotting system proteins. This leads to a temporary patch covering
and narrowing ( stenosis) within the artery lumen. Though this is
often a repetitive and progressive process over time, it is
typically without symptoms until a severe enough event, in a
critical enough area occurs.
Fibrous cap ruptures usually result in only a partial narrowing,
stenosis, of the artery lumen, a narrowing which usually partially
re-opens with healing and regrowth of the intimal lining. However,
sometimes the combination of atheroma material release, bleeding
into the atheroma bed, platelet accumulation and accumulation of
blood clotting proteins suddenly builds to the point of creating a
complete, or near complete obstruction. The obstruction, either at
the site of rupture, or as a result of debris sent downstream,
prevents adequate blood flow to cells downstream. Cells starved
for adequate blood supply are injured and may die.
Areas of severe narrowing, stenosis, detectable by angiography,
and to a lesser extent " stress testing" have long been the focus
of human diagnostic techniques for heart disease and
cardiovascular disease in general. However, these methods focus
only on detecting severe narrowing, not the underlying
atherosclerosis disease. As demonstrated by human clinical
studies, most severe events occur in locations with heavy plaque
yet little or no lumen narrowing present before debilitating
events suddenly occur. Plaque rupture can lead to artery lumen
occlusion within seconds to minutes, and potential permanent
debility and sometimes sudden death.
75% lumen stenosis used to be considered by cardiologists as the
hallmark of clinically significant disease because it is only at
this severity of narrowing of the larger heart arteries that
recurring episodes of angina and detectable abnormalities by
stress testing methods are seen. However, clinical trials have
shown that only about 14% of clinically debilitating events occur
at locations with this, or greater severity of narrowing. The
majority of events occur due to atheroma plaque rupture at areas
without narrowing sufficient enough to produce any angina or
stress test abnormalities. Thus, as of the later 1990s, greater
attention has been focused on the vulnerable plaque.
Though any artery in the body can be involved, usually only severe
narrowing or obstruction of some arteries, those which supply more
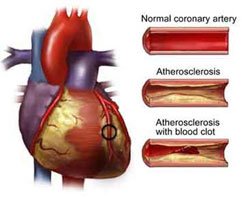
critically important organs, are recognized. Obstruction of
arteries supplying the heart muscle result in a heart attack.
Obstruction of arteries supplying the brain result in a stroke.
These events are life changing, and often result in irreversible
loss of function because lost heart muscle and brain cells do not
grow back to any significant extent.
CHIEF DISORDERS OF THE HEART
Atherosclerosis - treatment of Atherosclerosis,
Atherosclerosis types, Disease medicines, Atherosclerosis symptoms,
Atherosclerosis and Disease symptoms, Atherosclerosis symptoms Disease and
diagnosis, Symptoms and Solutions, Signs and Symptoms, type of
Atherosclerosis, cause common, common Atherosclerosis, Atherosclerosis List,
causes list, Infectious Atherosclerosis, Causes, Diseases , Types,
Prevention, Treatment and Facts, Atherosclerosis information,
Atherosclerosis: Definition, Atherosclerosis names, medical Atherosclerosis,
medical Atherosclerosis and disorders, cell Atherosclerosis, Atherosclerosis
Worldwide, Atherosclerosis Research, Atherosclerosis Control,
Atherosclerosis Center, Digestive Atherosclerosis Week, Information about
Atherosclerosis, causes of different Atherosclerosis, Atherosclerosis
Articles, Atherosclerosis and conditions, Health and Atherosclerosis,
Atherosclerosis Patients, Atherosclerosis and Sciences, causes of
alzheimer's Atherosclerosis, Atherosclerosis causes, alternative medicine
heart Atherosclerosis, body ailments, Atherosclerosis medicines, medical
antiques, type of blood Atherosclerosis